

Live. Laugh. Smile.
Crossbites
So you just finished your visit at the dentist and your daughter or son has no cavities! Amazing! But the dentist informs you that there is an issue with the jaw resulting in a crossbite and has referred you to office.
Firstly, there is no reason to worry. Crossbites are common and in some studies, they are shown to occur in up to 22% of the population. Secondly, crossbites are very easily corrected, and the earlier you correct them, the better!
What is a crossbite?
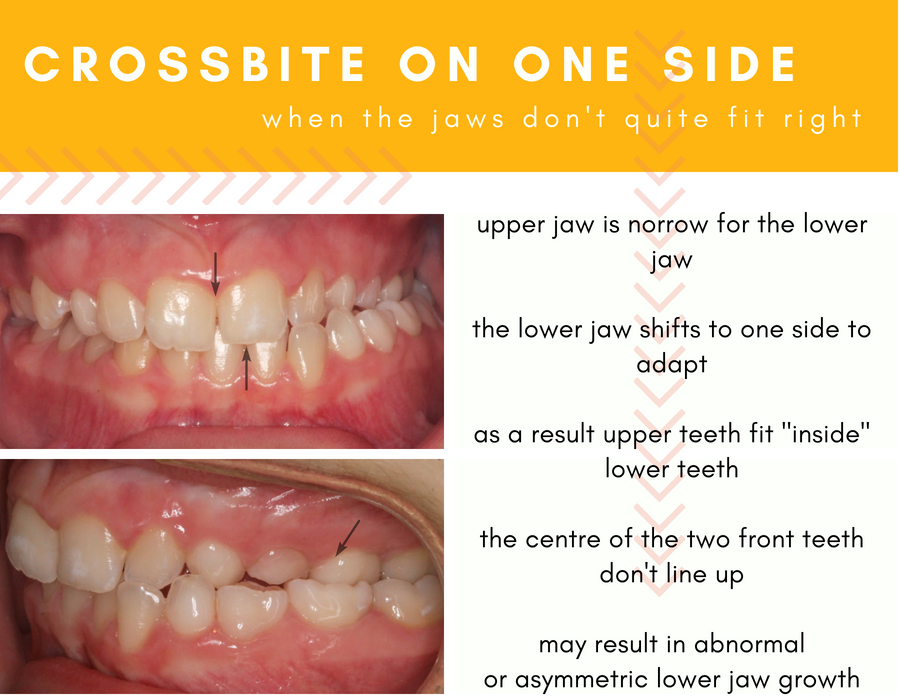
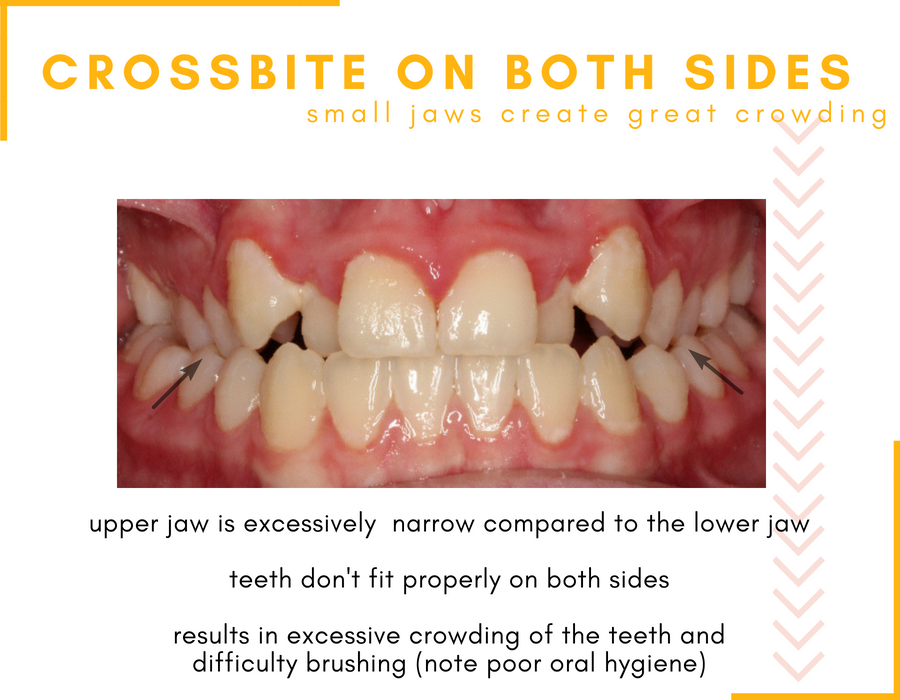
The most common type of crossbite occurs when the upper jaw is too narrow for the lower jaw. As a result, the upper molars and premolars (the back teeth) sit “inside” the lower teeth instead of sitting over top and slightly outside the lower teeth. When this occurs, it is called a posterior (in the back) crossbite. A crossbite can be unilateral (occurring only on one side) or bilateral (occurring on both sides). Sometimes, the opposite can occur where the lower jaw may be too small, although this is less common.
What causes crossbites?
There are several reasons that crossbites can present themselves. A lot of parents that come to our office think or feel that they did something wrong. We want to assure you that you did nothing wrong. Crossbites can be inherited and chances are that if you needed an expander when you were younger, so will your child. Crossbites can also be due to environmental factors including: finger or digit sucking habits, pacifier use, large adenoids or tonsils or allergies that result in mouth breathing. Studies have also shown that those who have been intubated during infancy also have a significantly higher prevalence of crossbites.
Why is it important to correct a crossbite?
Imagine you borrowed your friends shoes to play a game of basketball and they were slightly too small. After about an hour of playing, your feet start to hurt and by the end of the game you end up with calluses and blisters. If you were to wear these shoes over days, weeks and months, you may develop bunions, redness, and inflammation, which ultimately could affect the health of your feet and associated joints. This is an oversimplified analogy but it demonstrates that if parts of the body don’t fit quite right, a domino effect is created for other possible complications to arise in the future.
The same is true when the upper and lower jaws don’t fit properly. When the upper jaw is too narrow for the lower jaw, in order for the back teeth to touch, the lower jaw has to shift either to the right or the left so that the back teeth can touch together and function for chewing and grinding food. However, if the lower jaw has to compensate for the size of the upper jaw by shifting in one direction, this means that it is not sitting properly within its joint cavities. If you look closely, the chin will either be to the right or the left of the middle of the face – resulting in an asymmetry of the face. Because the lower jaw is not sitting properly in its joints, this may lead to temporomandiublar joint disorders or issues with the joints of the lower jaw.
Many studies show that if left untreated, muscle, skeletal and joint adaptations occur as a result of crossbites lead to permanent growth alterations and facial asymmetries.
How are crossbites treated?
Crossbites are generally treated with a device called a rapid palatal expander. There are several types of expanders: Banded expanders, bonded expanders, Haas expanders and removable expanders, each with their advantages and disadvantages.
The upper jaw is divided by soft fibrous tissue called a suture. This tissue starts to close and become bone at around 12 years of age. Expanders take the advantage of a child’s natural growth and help to widen the upper jaw to its natural size, when the suture is still soft.
What types of expanders are there?
Each expander consists of a screw that is stabilized by the back molars. The screw is turned by a parent each day until the crossbite is corrected. Whether your expander treatment is being carried out in our Mississauga or Sudbury office, you are seen by Dr. Virdee every four weeks to make sure that everything is going according to plan.
Banded Expanders
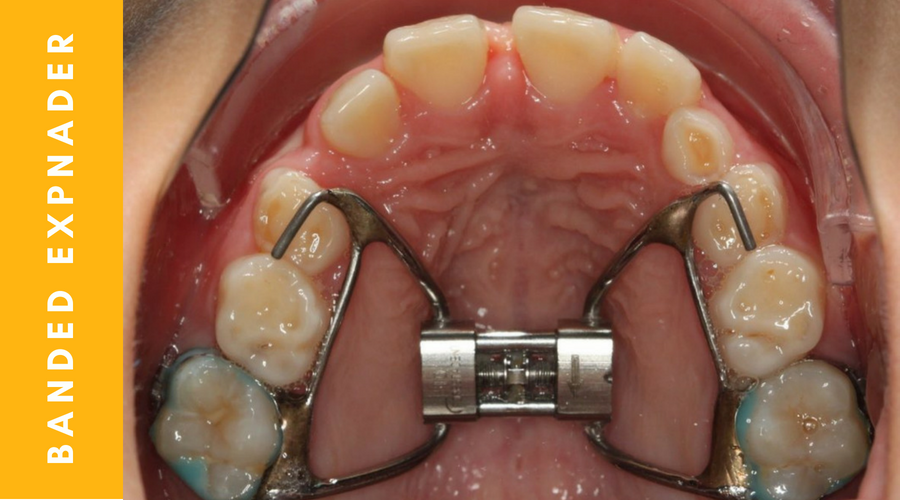
Banded expanders are the most streamlined expanders that are used. These expanders are stabilized by the back teeth, allow for greatest access to oral hygiene and are most cost-effective. Because they are semi-permanent, treatment time is shorter and results are more stable over time compared to removable expanders. We use this type of an expander in 99% of our offices.
Bonded Expanders
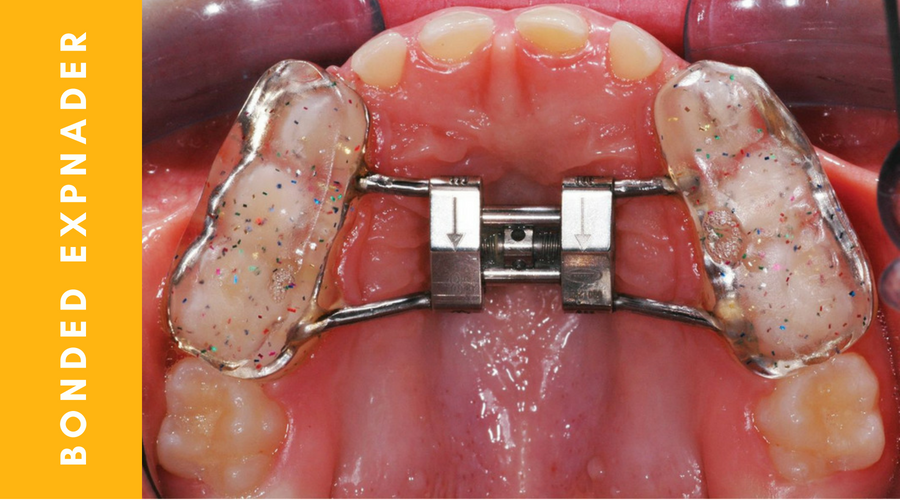
Bonded expanders are used when the upper teeth are covered excessively by gingiva making it difficult to fit a banded expander. In this case, acrylic covers the first permanent molars and the baby teeth. Like the banded expander this expander is semi permanent, and the results are more stable with shorter treatment time than removable expanders. Access to oral hygiene is difficult with this expander. We occasionally use this type of an expander in our offices.
Hass Expander
A Haas expander looks like a banded expander except it has acrylic coverage on the palate (roof of the mouth). This type of expander is semi-permanent and therefore delivers short treatment times and stable results. However, oral hygiene is very difficult which is why we do not use this appliance. P.S. Studies have shown no difference between the banded expander and the Haas expander – so why use something that creates a foul odour in the mouth!
Removable Expander

A removable expander have an expansion screw and is anchored to the teeth by clasps. Dr. Virdee follows an evidence based approach to orthodontic treatment. Studies have shown that removable expanders have poor compliance (i.e. patients don’t wear them very well) which results in relapse (the crossbite returns after treatment) and low success rates (stable expansion is rarely stable over time). This results in increased treatment time and increased cost (due to poor compliance and lost appliances).
How long does the expander stay in the mouth for?
Typically expansion therapy lasts 7-8 months. There is usually 1-2 months of active turning of the appliance. Remember, when you are turning an expander you are separating the two halves of the upper jaw. If you remove the expander too soon, and the bones have not had time to mature, the upper jaw shrinks back to its original size. It takes approximately 6 months for the bones to mature after the last turn is completed, which is when removal is recommended.
Why should expansion be completed earlier than later?
>
Remember, in young children, the upper jaw is divided in half by soft fibrous tissue called a suture. This suture starts to convert into bone at around 12 years of age. Because expanders are connected to teeth, when you start turning the expander you will also see movement of the back teeth towards the cheeks. The movement of the teeth is less desirable because once your remove the expander, the teeth shift back. Therefore, you want to maximize the separation of the bones (skeletal expansion) and minimize the movement of the teeth (dental expansion).
What are the benefits of palatal expansion?
When expansion is done is younger children, the suture is softer and you will get more bony or skeletal movement. As a child matures, expansion becomes more difficult and possibly more painful because the suture is more developed with bone. You will still get separation of the bones and widening of the upper jaw, but this will be accompanied by the less desirable, outward movement of the teeth. This means, the patient is in treatment for a longer period of time and the results are less stable.
Other benefits of expansion
- More space for adult teeth means less chance of extractions and tooth impaction requiring surgical intervention
- Improved nasal breathing
- Less chance of permanent asymmetries of the face
How will expansion change my child’s day to day life?
Like anything new, your child has to get used to the expander in their mouth. The good news is, because children are more resilient than adults, it’s easier for them to get used to something new. It usually takes about a week to get used to eating, chewing and speaking with the appliance. When you first start turning the expander, there may be pressure between the two front teeth and a possible gap may develop. We LOVE to see this as orthodontists because this means that the expander is working. Overtime this gap usually closes on its own as the teeth move towards each other. There may also be pressure of the back teeth, but this only occurs in the first couple of turns.
Why does Dr. Virdee sometimes recommend an expander for the lower jaw and the upper jaw?
In patients who have significant crowding of the upper and lower jaw without a crossbite, we may do treatment with both upper and lower jaw expanders. Remember, expansion doesn’t only correct crossbites, it also helps to create space for adult teeth to erupt. If your child comes in with a good bite (no crossbite), but with significant crowding, we will first expand the lower jaw to create space for adult teeth to erupt. After three months, this will be followed by expansion in the upper jaw, again to create space. Completing expansion in both the upper and lower jaws ensures that the upper and lower teeth fit properly before and after treatment.

What else should I know about expanders?
Whether your child has and bonded expander or a banded expander, if you have any questions, know that we are always here to answer them. Expansion therapy is one of the best type of orthodontic treatments that can be completed for a patient (but only when done using a semi-permanent expander). It has very small side effects (if any) and the benefits are tremendous. Remember, Dr. Virdee’s treatment recommendations are always backed by science. If you need more information about any of questions above, read this article: https://www.cda-adc.ca/jcda/vol-71/issue-8/569.pdf.
Smile Gallery
-

Correction of a crossbite with an expander
Alexa had a crossbite on the left hand side and crowding of the upper from teeth. Expansion of the upper jaw corrected the crossbite and created enough space for the upper front teeth to erupt and align naturally without using braces.
Total treatment time: 8 months
-

Correction of a crossbite and tongue thrust with an expander
Zoe had a crossbite on both sides. She also had an open bite (gap between the upper and lower front teeth) due to a tongue habit. She was treated with an expander in combination with a tongue crib to help with her tongue habit. The upper jaw was expanded to correct the crossbite and the open bite spontaneously resolved itself once the tongue habit was corrected.
Total treatment time: 8 months
-

Correction of a crossbite with an Expander
Julia had a crossbite on the right hand side with crowded upper front teeth which were difficult to keep clean (notice that the gingiva is slightly overgrown and red before treatment). Expansion of the upper jaw corrected the crossbite and helped to resolve the crowding of the upper jaw naturally without the use of braces which helped with better gingival health.
Total treatment time: 8 months
-
Correction of a crossbite with an expander
Alexa had a crossbite on the left hand side and crowding of the upper from teeth. Expansion of the upper jaw corrected the crossbite and created enough space for the upper front teeth to erupt and align naturally without using braces.
Total treatment time: 8 months
-
Correction of a crossbite and tongue thrust with an expander
Zoe had a crossbite on both sides. She also had an open bite (gap between the upper and lower front teeth) due to a tongue habit. She was treated with an expander in combination with a tongue crib to help with her tongue habit. The upper jaw was expanded to correct the crossbite and the open bite spontaneously resolved itself once the tongue habit was corrected.
Total treatment time: 8 months
-

Alexa
-

Zoe
-

Julia
-
Alexa
-
Zoe
Get a Free Consultation
Make an appointment today and start your child’s journey to a healthy and beautiful smile with Hometown Orthodontics.